National Stroke Audit Development

National Stroke Audit Development
Acute stroke services framework. P 17 shows how it was developed with reference to other entities but it is clear that the framework is the creation of the S.F. who reviews its contents biennial issue.
Moving onto “Table 1 National Adherence to the Acute Stroke Clinical Care Standard Indicators”, get your copy of “Acute Services Report 2017” as I intend only to examine entries of particular interest. There is a point of reference to show what facilities are available in stroke units and how patients are guided through the system.
One entry that puzzles me are numbers after the description entries.
- Thrombolysis in ischemic stroke 131 1369 “this seems an absolutely low number from 31,951 acute stroke submissions. I remember some years ago when alteplase was first used, N.S.F articles reported the low use of this clot bluster one person suggested an aim of 20 P.A. many comments in the report have been pasted from previous publications, “with exclusions” is added to the description.
See later (2) “assessment by a physiotherapist within 48 hours of hospital admission. This is within the 3 day limit for upper limb therapy, but it has to be continued for the length of hospital stay. This is covered in the next entry (3) “treatment for a rehabilitation goal commenced during acute hospital admission” clear.
(4) “Discharged on antihypertensive medication (intracerebral hemorrhage)”
(4 A) no mention of a neurological surgeon- the only stroke unit members qualified to put in temporary or long term blood drainage tubes and repair vascular tears and leaks. So our critical patients are sent off with blood pressure pills.
(5) “Discharged on statin, antihypertensive and antithrombotic medications (Ischemic stroke)”
(4 A) how on earth does any stroke audit based on clinical care standard indicators limit any reference to brain bleeds to one line without mention of known therapy efforts. About 20% of strokes are said to be due to brain vascular problems, and, I believe, with more serious adverse consequences, everyone knows of the approx. death rate of 20%. Do we think this could be due to leg weakness due to latest thrombolysis or to a massive brain vessel bleed? Anyone for a research?
(6) Discharge of medication for A.F
(7) “Education about behavior changes for modifiable risk factors”
(8) “Care support needs assessment”
(9) “Carer training”
(10) “Written care plan”
(5A) “Statin”. Use of named meds is to be avoided. What happens when a respondent agrees with everything except that word?
(7A) This requires a psychologist to be on staff
(8A) Who will assess care support? Physios?
(9A) Carer training who knows what they do?
(10A) Written care plan for patients this sounds like a joint job for nurses, social workers and physios.
Now we come onto the concept of the framework. “Cover everything from ambulance to hospital treatment to home”. Which I assert is an impossible task. It breaks down when Carer activities are included in the framework.
Disclosure: I was admitted to an acute hospital in 2012 with stroke, caused by a clot- successfully cleared. I was unconscious for maybe four days during which time meds were changed up or down till I was stabilized and given a recovery bed. It was made clear that I would be discharged 30 days after admission. A social worker helped find a rehab hospital. Therapy was minimal while I waited.
It should be obvious that acute hospitals which take all A&E people who turn up and which are financially constrained for long patient stays are not suited for Carer work which can last the life of the S.A.P.
However, carers are being included in NAT. stroke audits.
Independent living the RANKIN SCORE, a commonly used scale for measuring the degree of disability or dependence in the daily activities of people. A must for people who use the phrase independent living
Ref. National Stroke Audit- Acute Services Report 2017 P.45
67% of SAP live at home with others.
24% lived alone.
CONCLUSION
Neuro nurses, social workers, and physios all have well understood parts to play in stroke patient care. It seems to me that there is ample evidence to conclude that these carers are just an unnecessary concept.
Thrombolysis Indicators
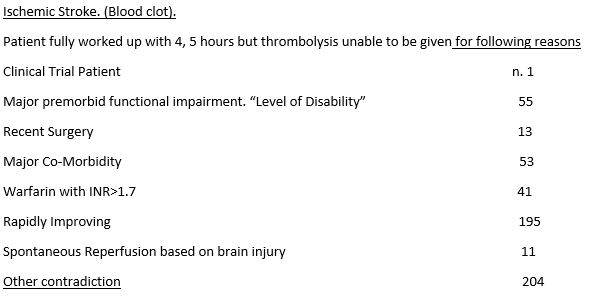
No wonder thrombolysis usage is stuck on 15.% I have been using meds which supersede warfarin for about 20 years.
Stroke Audit
To S.F.
Thanks for letting me see the stroke audit. I do not want to see any further issues. Careful angiography. The term C.T. angiography caused me to think. This is just the routine injection of contrast medium to see if any stray blood is loose in the brain, indicating no clot busting injection. Could the first standard C.T. miss a small but weak aneurism tucked between brain flaps which could burst if the contrast injection was set too high a pressure?
I suggest that the stroke team discuss this with the consulting radiologist, who should be regular at the stroke team.
Enough.
Angus